The 2016 Legislature is currently holding hearings on proposed Medicaid Buy-In Legislation. If you support a Medicaid Buy-In, you can submit testimony and view the measure status using the links below.
You can also show support by contacting the office of the Governor.
The Honorable David Ige
Governor, State of Hawai’i
Executive Chambers, State Capitol
Honolulu, Hawai’i 96813
Phone: 808-586-0034
Fax: 808-586-0006
Medicaid Buy-In Participation by State
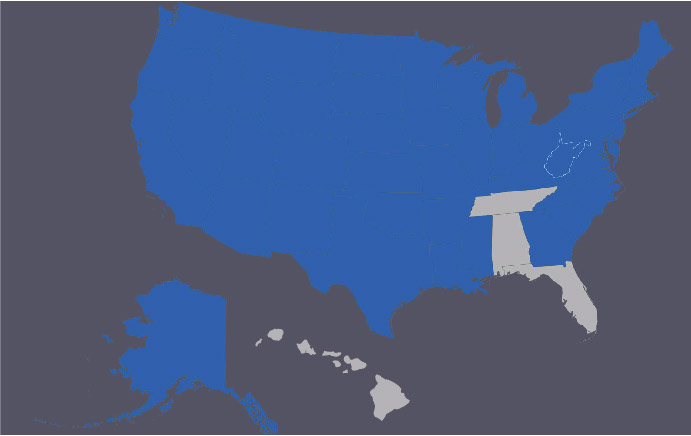
Let’s Make Hawaii the 47th State with MBI!
Background
Working-age adults with disabilities need adequate health insurance to enter or remain in the work force, but their options for insurance coverage are limited. Many who have full-time jobs may not be covered through their employer-sponsored health insurance because of a pre-existing condition. Those who work part-time or have jobs that do not offer health coverage may have to turn to government-sponsored programs, such as Medicaid. However, a person with a disability who earns more than the allowable amount will be ineligible for Medicaid coverage. That’s where the Medicaid Buy-In program comes in.
A Medicaid Buy-in enables people with disabilities to work and use Medicaid by “buying in” (i.e., by paying a premium and/or cost-share.) On July 6, 2012, Governor Abercrombie signed HB 2415 into law to establish a task force to implement a Medicaid Buy-in program in Hawai‘i.
The Medicaid Buy-In program allows adults with disabilities to earn more than would otherwise be possible and still have Medicaid coverage. In return, participants “buy into” the Medicaid program, typically by paying premiums based on income. As of June 2012, 45 states were operating a Medicaid Buy-In program to extend Medicaid coverage to working people with disabilities, with total nationwide enrollment of more than 100,000. (Mathematica Policy Research)
Why Hawaii needs a Medicaid Buy-In:
- A Medicaid Buy-In Program in Hawaii can generate $240,000 fiscal benefit to the State in its first year of implementation.
- $2.3 million fiscal benefit to the State over 5 years.
- Medicaid Buy-In beneficiaries are more likely to have Medicare, (80% or more).
- Savings on SNAP can reach over $70,000 in first year, and $700,000 over 5 years.
- Governor Abercrombie sponsored Medicaid Buy-In program in US Congress under the Ticket to Work in 1999.
- Less than 70% of Medicaid Buy In recipients are already known to Medicaid.
- Generates revenue of $80,000 in General Excise Tax in its first year, and more than $750,000 over 5 years.
- 45 States have Medicaid Buy-Ins.
- State Medicaid officials may customize Buy-Ins to fit the state’s overall healthcare strategy
- Medicaid Buy-In could generate $100,000 in premium in its first year and $900,000 over 5 years
Policy Brief
MEDICAID INFRASTRUCTURE GRANT – HAWAII POLICY BRIEF
HIRE ABILITIES – QUEST WINS – WORK INCENTIVE NEW START
PERSONS WITH DISABILITIES IN HAWAII
In Hawaii, there are approximately 22,000 adults receiving SSDI benefits as “disabled workers”; the average benefit for a disabled worker is about $1,097 per month. SSDI recipients get Medicare after a 2-year wait, but many need medications and other assistance not covered by Medicare.
- get Supplemental Security Income;
- get Home and Community Based Services (HCBS) or facility care; or
- have enough medical bills to spend their income down to qualify for short-term coverage through the state’s Medically Needy Program.
- 69.6% of respondents would sign up for a premium sharing program that would allow for work without losing healthcare benefits;
- 82.4% of respondents expressed interest in information about how to find and keep a job without losing healthcare benefits;
- Lack of job supports, such as assistive technology and personal assistance, and the potential loss of benefits dissuade people with disabilities from working.
- reduce the number of uninsured or underinsured persons in Hawaii;
- remove documented barriers to work, such as loss of benefits, lack of job supports and personal assistance services, and being told not to work by case workers;
- help working people with disabilities increase their economic independence and live above poverty by providing needed health care coverage and decreasing their reliance on SSDI or SSI benefits;
- enable some SSDI recipients to work and get Medicaid as a supplement to private or Medicare insurance;
- obtain federal funding for health care services for persons now served through state-funded mental health programs; and
- allow persons with disabilities to work and pay state, federal and FICA taxes.
- for every $1.00 that the state spends on Medicaid, there is a business activity return of up $3.17;
- in FY 2005, there were an estimated 11,000 jobs created due to Medicaid spending, with total spending on wages of $466 million; and
- every $1 million spent on Medicaid results in $3.2 million in new business activity, 29.34 jobs created; and $1.2 million in new wages.
- be employed;
- be age 18 through 64;
- be ‘disabled’ but for the earnings limit under SSA rules (Ticket Act, Title II, Section 201 (a)(1)(C));
- have net countable income less than 250% FPL under the Social Security counting methodology. In 2011, this equals approximately $2,613/mo. of countable income, after Social Security disregards;
- have countable assets less than $20,000;
and - − pay a premium.
- Former 1619(b) Recipients and Others with earnings too high for Medicaid
- People with disabilities enrolled in Medicaid under a medically needy, spend down, or poverty level categories
- People with disabilities who lack other sources of health insurance, including SSDI beneficiaries in the 24-month waiting period before receiving Medicare, and working SSDI beneficiaries nearing the end of an extended period of Medicare coverage who will experience a loss of Medicare.
- People with disabilities whose premiums/cost sharing for other private or public insurance coverage (e.g., through private insurance, COBRA, spouses, or Medicare) exceed the cost of the QUEST WINS program.
- People with disabilities whose private and/or public (Medicare) coverage does not provide needed medical supports, but which are covered by the QUEST WINS program.
Hawaii Research
- Hawaii Medicaid Buy-In Proposal (.pdf)
- Hawaii Medicaid Buy-In Proposal (.doc)
- Hawaii Medicaid Buy-In Actuarial Pricing Analysis (.pdf)
Hawaii Testimony
- Testimony on SB126 (.pdf)